42,086 Is The Number
Governments around the world repeatedly told us the Covid jabs were "safe and effective". They compelled (or coerced via mandates) us to offer up our deltoids for a novel gene based medication to deal with a novel form of coronavirus (to be clear, the common cold is a coronavirus).
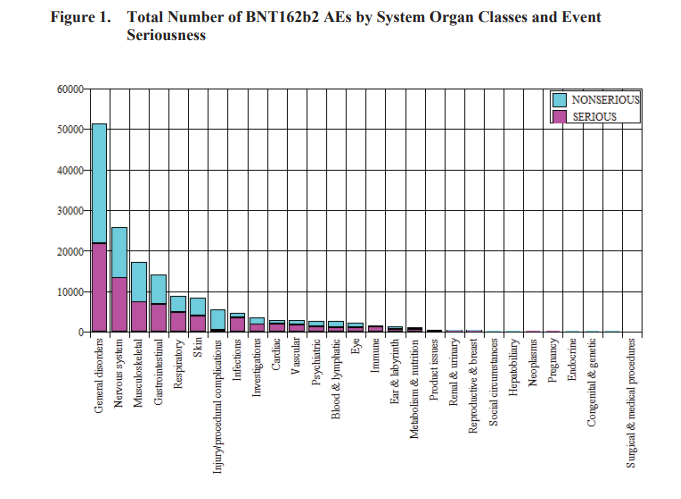
Using Pfizer's own documents, which they were forced to hand over by court order, we know that over the two month period the trials lasted 42,086 people suffered an Adverse Event of Special Interest (AESI). The proportion of serious Adverse Events (AE) are shown in the graph above. Almost half in each category, and sometimes a larger proportion when it comes to Cardiac and Vascular AE, were deemed serious.
What is unclear is the exact number of participants in the trials. In my article about the forced release of the trial documents I talk about this figure being redacted, which makes it hard to evaluate the exact rate of harm. Previously a drug with this level of AE would have been pulled off the market. This is what happened during the 2009/10 Swine Flu 'pandemic' and the rollout of Pandemrix. The UK Government lost the court case around 2017 and had to pay up to 60 people injured. The numbers of AE for the Swine Flu jab were a fraction of what we've seen with Covid jabs, even if we just count those injured in the trials.
There were lessons to be learned, and there's a good accounting here in the British Medical Journal from 2010. I suspect that in time similar conclusions will be drawn over the mass roll-out of the Covid jab with an examination of whose interests this really served.
in this recent story of swine flu, whose financial stakes for manufacturers the manufacturers did not even attempt to deny (see media on economy), nobody heard the manufacturers’ voices in the promotion of swine flu as a major threat to public health consisted entirely of national and international health or governmental agencies. This illustrates JK Galbraith’s recent thesis on The Predator State [8], namely that “deregulation” is not the law of jungle for the lobbies’ benefit, but the surrendering of the State’s power and prerogatives to those lobbies, whatever the cost to public health or finances
The full list of possible AE for the Covid jabs runs to roughly 9 pages. Click this link and scroll to the Appendix (page 30) for some sobering reading. While we might not know exactly the rate of harm, I would hazard a guess that the total number of trial participants would not be equivalent to the population of New Zealand. If over 42,000 people were harmed, many seriously, during the trials imagine how many in NZ have now had their health and lives ruined to save them from a virus, that even in it's earlier and more pathogenic form had a 99.97% survival rate for most of us who were young and healthy?
The average age of death from Covid was 82. Having worked in the aged care industry I can tell you that losing half a dozen or more elderly vulnerable people every year to flu or other viruses was a sad fact of life. And that was just the aged care company I worked for. The only thing unprecedented was that this time we locked down whole countries of healthy people and mandated a barely tested new medication with no long term safety data. They're now marketing it for healthy children who are not at risk from this virus. Again, whose interests would this serve?
The numbers of AE may be even worse. Pfizer trial AE were only observed for the duration of the trial. Many conditions can take months to emerge so people who subsequently suffered an AE outside the trial period may not have been recorded. We know that some AE were never followed up, even during the trials.
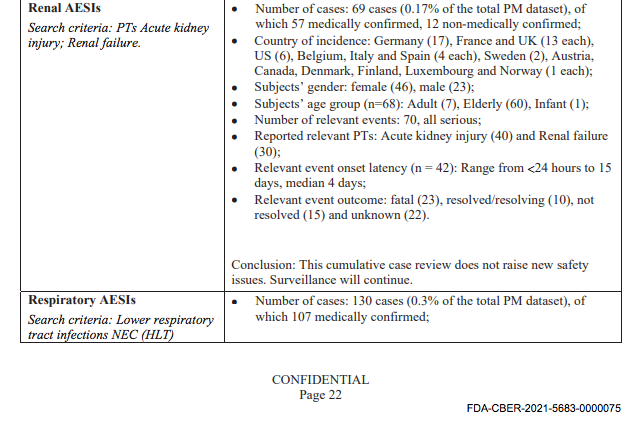
Take the above screen shot relating to Renal AESI. There were 69 cases of which 57 were medically confirmed and 12 non medically confirmed. Of that 23 were fatal, 10 resolved/resolving, 15 not resolved and 22 unknown. Meaning around 87% were either fatal, unresolved or unknown. They have no idea what happened to approximately 1/3 of the cases. Consider that this is just one of the possible AE. 61 people had a fatal stroke, 501 people had a neurological AE with 16 being fatal, 89 not resolved and 161..."unknown", for example.

The Pfizer trove of documents confirm earlier whistle-blower testimony, published in the British Medical Journal, alleging AE were not being followed up. Below is a quote from the BMJ investigative article summarising the shoddy research work carried out by Ventavia for Pfizer. Former Regional Director for Ventavia, Brook Jackson, alleged:
that the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial. Staff who conducted quality control checks were overwhelmed by the volume of problems they were finding.
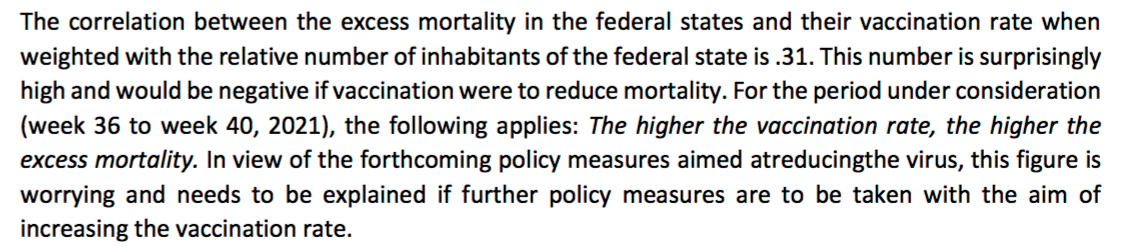
In every one of these AE of Special Interest Pfizer conclude that the "cumulative case review does not raise new safety issues." Inconveniently for Pfizer, new research into the alarming increases in Excess All Cause Mortality (non Covid deaths above the normal rate we expect each year) worldwide are rolling in. In a study of 16 federal states in Germany, for example, Professor Steyer and Dr Kappler crunched the numbers and concluded:
It is worth noting that Germany has very recently moved to publish their rate of jab injury (see here also for a short video regarding the rates of injury in Germany). NZ's current Government is still indulging in gas-lighting telling formerly healthy people injured that it's anything but the jab before adding-insult-to-injury by victim blaming.
In a January 2022 article in the BMJ, this author noted the following statistics:
The national Covid Actuaries Group reported at the end of 2021 that “Latest ONS deaths data (to week ending 17 December) showed that for England and Wales, 1,650 more deaths were recorded in-week compared to the 2015-19 year average. That’s 15% higher.”
The author puts it down to hospitals under pressure with staff shortages etc, pointing to a similar scenario in 2015. However, other researchers are also crunching the numbers and looking for patterns that might explain such rises in Excess All Cause Mortality, in Scotland, for example.
Professor Richard Ennos acknowledges that a plausible explanation may indeed be a health system under pressure, normal medical care not being given and people not accessing care when they need it. So lack of medical care is one hypothesis (scientific assertion to be tested). An alternative hypothesis is that there may be a relationship between excess death and the roll out of vaccines. Professor Ennos had observed that there was a 12 - 14 week delay between the rollout of vaccines to a particular age group and increase in death rate.
What we can do is we can run an experiment and the [Scottish] Government have run an experiment and the experiment is that we apply what we think might be causing the excess deaths, and that is the vaccines. So we give a booster dose of the vaccines and if our hypothesis about excess death being caused by vaccines is correct we should see a rise in deaths about 12 - 14 weeks after the application of those experimental vaccines.
In the beginning of 2022 we didn't have excess deaths, excess deaths held, but then it started again, in Scotland. It started about 10 weeks into 2022 and it started first in the older age groups and then it started later on in younger age groups. That's exactly as we would predict according to our hypothesis that there is some relationship between excess death and vaccines.
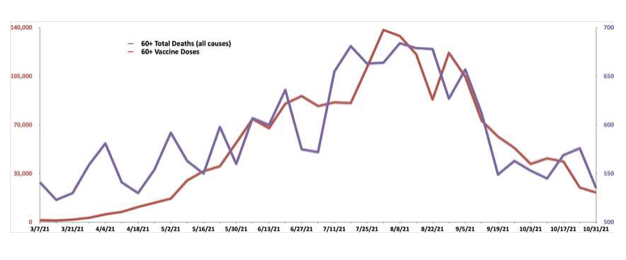
While the fixation on Covid, suspension of normal medical screening and the sustained fear campaign around not overwhelming the hospital system may be a factor, research by people like Professor Ennos paints a more damning picture that is hard to dismiss with the wave of a hand. Need I make the point that deaths are happening outside the 8 week duration the trials lasted? Closer to home in NZ, Dr. Guy Hatchard details similar findings by Grant Dixon showing a relationship between jab roll-outs and excess death for those 60+. The graph below was based on data that had to be gained via OIA.
New Zealand is a small place so anecdotally most are aware of people in their circle who have suffered one of the myriad of AE listed. I personally know of a Bells Palsy immediately after the booster, which was never recorded officially as many AE are not, a suspected Pericarditis (fortunately recorded), two cases of Shingles (suggestive of lowered immunity) and 'migraine' so severe it required hospitalisation.
I've heard others talk about sudden and unexpected heart attacks and strokes in people either too young or healthy to be getting either. Sudden Adult Death Syndrome (SADS) is suddenly a thing, but we're told to ignore it because young people have always dropped dead or just not woken up in large numbers, eh?
We are now reaping what panicked and/or opportunistic Governments, who were clearly in the grip of Global Group Think, have sown!
How the New Zealand Government, aided by a paid off media and censorship via Big Tech, has managed to downplay any suggestion of AE being a real and present risk is in itself remarkable, in a most malign way. The dam is breaking though and they're only stalling the inevitable reckoning.